

Cord Blood vs. Bone Marrow: Recovery and Complications
When deciding between cord blood and bone marrow transplants, the key differences lie in recovery time, risks, and availability. Here's a quick breakdown:
- Cord blood transplants: Slower initial recovery (neutrophil recovery in 19–27 days), higher risk of early infections, but lower risk of chronic Graft-Versus-Host Disease (33% vs. up to 71% for bone marrow). Cord blood is ready for immediate use and tolerates genetic mismatches better.
- Bone marrow transplants: Faster recovery (neutrophil recovery in ~18 days), higher risk of GVHD, and requires finding a compatible donor, which can take months.
Quick Comparison:
| Metric | Cord Blood Transplant | Bone Marrow Transplant |
|---|---|---|
| Neutrophil Recovery | 19–27 days | ~18 days |
| Platelet Recovery | 40–60 days | 27–29 days |
| Full Immune Recovery | 6–24 months | 6–18 months |
| GVHD Risk | Lower (33%) | Higher (52–71%) |
| Availability | Immediate (stored) | 4+ months (donor search) |
Cord blood is ideal for urgent cases or when a donor match isn't available. Bone marrow offers faster recovery but comes with higher GVHD risks. Both options have pros and cons, and the choice often depends on timing and patient-specific factors.
Cord Blood vs Bone Marrow Transplant Recovery Times and Complication Rates
Cord Blood Transplant Recovery Times
Engraftment and Immune Recovery Phases
The recovery timeline for cord blood transplants stands out for being slower and more gradual compared to other methods. The first key milestone, known as neutrophil recovery - when white blood cells start functioning again - has a median time of 23 days post-transplant. However, this can range widely from 11 to 133 days. For comparison, bone marrow transplants average 21 days, while peripheral blood stem cells typically take just 16 days.
Recovery unfolds in a specific order: monocyte engraftment occurs within about two weeks, followed by neutrophil recovery (median 23 days). Natural killer (NK) cells increase shortly after, B-cell recovery happens between 3 and 12 months, and T-cell reconstitution can take anywhere from 6 to 24 months. Although some T-cell subsets recover within 100 days, naive CD4+ and CD8+ T-cell levels often stay low for at least 6 months to a year. A fully reconstituted immune system generally takes 6 to 24 months, provided complications like graft-versus-host disease (GVHD) don’t interfere.
During the first 30 days, patients are at high risk for bacterial and fungal infections. Between days 30 and 100, viral reactivations - most notably CMV and HHV-6 - become a concern, with HHV-6 reactivation occurring at a median of 26 days. This particular virus has been linked to an increased risk of primary graft failure in cord blood transplants.
Several factors influence these recovery phases, as detailed below.
Factors That Affect Cord Blood Recovery
Recovery speed is closely tied to the cell dose used in the transplant. For successful engraftment, a minimum dose of 2×10⁷ cells/kg is recommended. Higher counts of CD34+ cells or T-cells can accelerate both engraftment and immune system recovery. When a single cord blood unit lacks enough cells, doctors may opt for a double cord transplant to meet the necessary dose.
Other critical factors include HLA matching, which improves immune recovery and reduces the likelihood of graft rejection. While cord blood transplants are more tolerant of mismatches than bone marrow transplants, better matching still leads to better outcomes. Age also plays a role - older donors or recipients may experience slower recovery due to aging marrow or thymic atrophy, which limits T-cell regeneration. The intensity of the conditioning regimen (chemotherapy or radiation) can speed up engraftment but may slow early lymphocyte recovery. Advanced processing techniques, like Americord’s CryoMaxx technology, aim to maximize stem cell yield and improve recovery results.
Bone Marrow Transplant Recovery Times
Bone marrow transplants follow a unique recovery process that differs from cord blood transplants.
Recovery Milestones
The recovery timeline for bone marrow transplants begins as soon as stem cells are infused. The process kicks off with the conditioning phase, lasting 1–9 days, during which high-dose chemotherapy or radiation is used to eliminate cancer cells and prepare the bone marrow. Stem cell infusion happens on Day 0 through a central venous catheter.
Once infused, the new stem cells migrate to the bone marrow and start producing blood cells within 2–6 weeks. Hospital discharge typically occurs when key blood count thresholds are met: an absolute neutrophil count of 500–1,000/mm³, a platelet count of 15,000–20,000/mm³, and a hematocrit level of 25%–30%. For autologous transplants (using the patient’s own cells), hospital stays average about 2 weeks, while allogeneic transplants (using donor cells) require 3–4 weeks due to the need for closer monitoring for complications.
The first 100 days post-transplant are critical, requiring frequent outpatient visits and close monitoring, especially in allogeneic cases due to the higher risk of graft-versus-host disease (GVHD). Immune recovery takes about 6–12 months for autologous transplants and 1–2+ years for allogeneic transplants. During this time, blood counts stabilize, and patients must follow a new vaccination schedule, as the transplant erases previous immunities.
How Transplant Type Affects Recovery
The type of transplant significantly impacts recovery duration and complexity.
Autologous transplants use the patient’s own stem cells, which eliminates the risk of GVHD. This leads to a simpler recovery process, with immune function typically restored within 6–12 months. However, these transplants lack the "graft-versus-cancer" effect, where donor cells can help target remaining cancer cells.
Allogeneic transplants, on the other hand, use donor cells, which introduces both advantages and challenges. While the graft-versus-cancer effect can be a powerful tool against cancer recurrence, these transplants come with a higher risk of GVHD. Patients often require immunosuppressive medications, which slow immune recovery and increase vulnerability to infections. Full immune recovery can take 1–2+ years, and patients face ongoing risks until they’ve been off immunosuppressants for at least two years without active GVHD. For older patients, reduced intensity conditioning (RIC) transplants - using lower doses of chemotherapy - can be an option, though recovery timelines remain comparable.
These differences in recovery timelines and risks play a crucial role in shaping patient outcomes and overall quality of life.
| Recovery Milestone | Autologous Transplant | Allogeneic Transplant |
|---|---|---|
| Average Hospital Stay | ~2 weeks | 3–4 weeks |
| Engraftment Period | 2–6 weeks | 2–6 weeks |
| Intensive Monitoring | First 30–100 days | First 100 days |
| Full Immune Recovery | 6–12 months | 1–2+ years |
| Primary Risks | Graft failure, infection | GVHD, infection, rejection |
These distinctions highlight the complexities of recovery and set the stage for comparing clinical outcomes in the next section.
Recovery Time Comparison
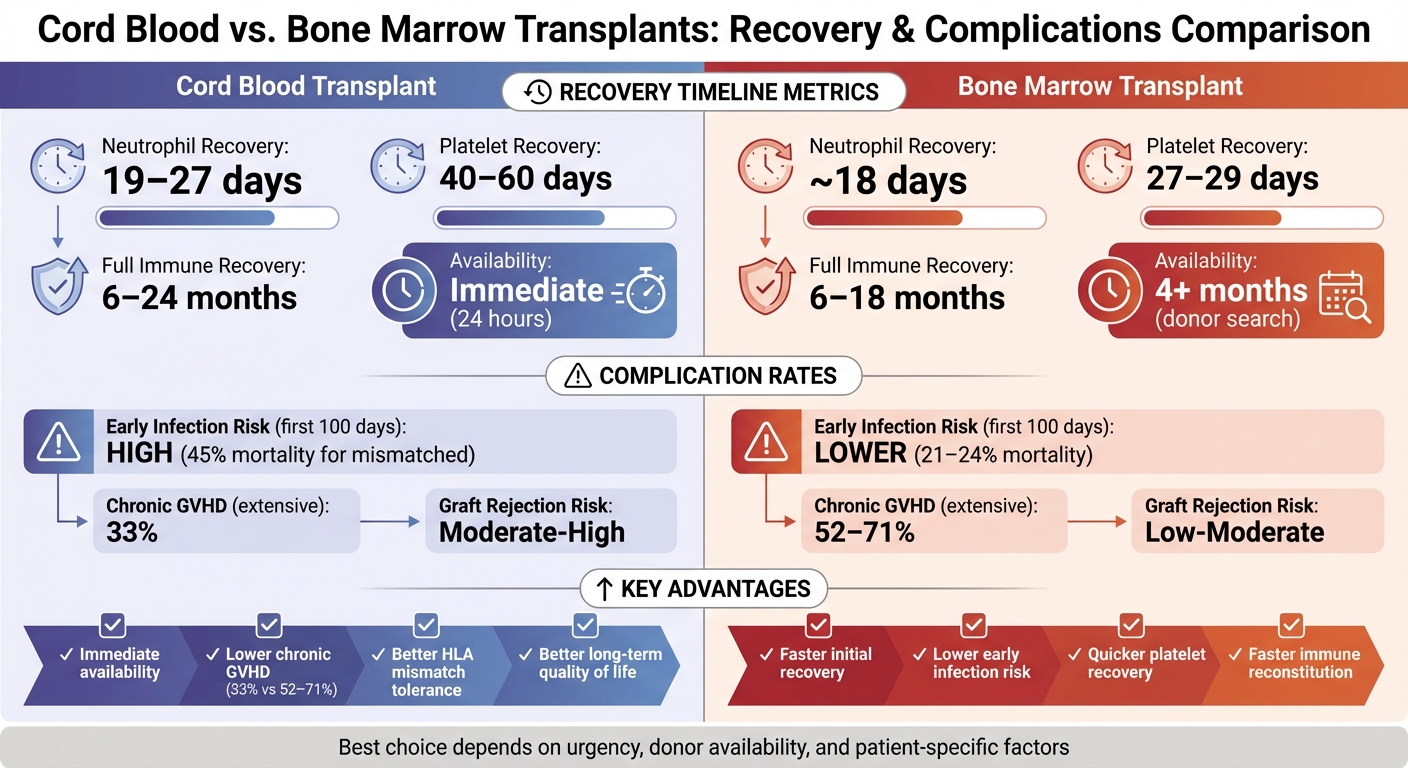
Cord blood transplants generally take longer for initial recovery compared to bone marrow transplants. For example, neutrophil recovery with cord blood transplants typically happens within 19–27 days, while matched bone marrow transplants achieve it in about 18 days. Similarly, platelet recovery takes 40–60 days for cord blood transplants, compared to just 27–29 days for bone marrow transplants.
This slower recovery is primarily due to the lower total nucleated cell counts in cord blood. However, cord blood has a major advantage: it’s ready to use almost immediately. Cord blood units can be shipped and prepared for transplant within 24 hours. In contrast, finding and coordinating with a bone marrow donor can take over four months - a delay that could be critical for patients battling aggressive cancers.
Side-by-Side Recovery Metrics
| Metric | Cord Blood Transplant | Bone Marrow Transplant (Matched) |
|---|---|---|
| Median Neutrophil Recovery | 19–27 days | 18 days |
| Median Platelet Recovery | 40–60 days | 27–29 days |
| Full Immune Recovery | 6–24 months | 6–18 months |
| Availability Timeline | Immediate (ships in 24 hours) | 4+ months (donor search) |
Over time, the recovery gap between these two approaches narrows. Cutting-edge advancements like Notch-mediated expansion and copper chelation are helping to overcome the low cell dose issue in cord blood transplants. These innovations are speeding up myeloid recovery and bringing engraftment times closer to those of bone marrow transplants.
For patients needing urgent transplants or those unable to find a suitable bone marrow donor, cord blood's rapid availability can be a game-changer. As expansion technologies continue to improve, the choice between these two options becomes increasingly dependent on individual circumstances and timing needs.
Cord Blood Transplant Complications
Early and Long-Term Risks
Cord blood transplants come with notable early risks. One key issue is prolonged neutropenia, a condition where white blood cell levels drop dangerously low, leaving patients highly vulnerable to infections. While neutrophil recovery generally happens around day 23, recovery times can vary widely - from as little as 11 days to as long as 133 days.
This extended neutropenic phase significantly raises the risk of infections. A study conducted between January 2006 and December 2015 by researchers at the University of Michigan Health System and Karmanos Cancer Center tracked 57 adult cord blood transplant recipients. They recorded 179 infectious episodes, with 41% occurring within the first 30 days. Among the 10 patients who never achieved neutrophil engraftment, 9 died within 100 days, with infection being the cause of death for 6 of them.
"Infection is estimated to cause 35%–50% of nonrelapse mortality in patients after UCBT, compared with 8%–22% after allogeneic HCT." - Kathleen A. Linder, Division of Infectious Diseases, University of Michigan Health System
Another significant concern is graft failure, which occurs when blood counts fail to recover within 7 weeks. This risk increases in cases of donor-recipient mismatches or when a single cord unit with low stem cell counts is used. Other complications include Sinusoidal Obstruction Syndrome (SOS/VOD), a liver condition seen in 15%–40% of pediatric myeloablative transplants, and Transplant-Associated Thrombotic Microangiopathy (TA-TMA), which affects roughly 19% of recipients and has a 20% treatment-related mortality rate within the first 6 months. Despite these challenges, cord blood transplants offer benefits when it comes to long-term complications.
One key advantage is the reduced risk of severe chronic Graft-Versus-Host Disease (GVHD). Among patients who develop chronic GVHD, only 33% of cord blood recipients experience extensive disease. This is significantly lower compared to 52% for matched bone marrow recipients and 71% for mismatched bone marrow recipients. This reduced severity is attributed to the immunological immaturity of newborn stem cells, which are less likely to aggressively attack the recipient's tissues. This long-term benefit plays an important role in the overall appeal of cord blood transplants.
Bone Marrow Transplant Complications
Common Complications and Long-Term Effects
Bone marrow transplants, while life-saving, come with their own set of challenges, especially when compared to cord blood transplants, which are associated with lower rates of chronic GVHD. One of the most common and serious complications is Graft-Versus-Host Disease (GVHD).
This condition arises when the donor's immune cells attack the recipient's tissues. Acute GVHD affects up to 47% of allogeneic transplant recipients within the first 10–100 days and primarily targets the skin (causing rashes and burning), gastrointestinal tract (leading to severe diarrhea and nausea), and liver (resulting in jaundice). Chronic GVHD, on the other hand, develops in up to 50% of recipients between 100 and 600 days post-transplant and can cause ongoing issues like dry eyes, thickened skin, and joint pain.
Infections are another major concern. These can occur at any stage of recovery and are responsible for 4%–20% of late post-transplant deaths. The immune system often takes 9–24 months to recover fully after an allogeneic transplant, leaving patients vulnerable to bacterial, viral (such as CMV, EBV, and Adenovirus), and fungal infections.
Another complication, Sinusoidal Obstruction Syndrome (SOS) - also known as Veno-Occlusive Disease - affects 5%–15% of allogeneic transplant recipients, typically within the first three weeks. Symptoms include weight gain, fluid retention, and jaundice. Additionally, Transplant-Associated Thrombotic Microangiopathy (TA-TMA) occurs in about 19% of recipients and is linked to a significantly higher mortality rate due to treatment complications.
Long-term effects can also be profound. Survivors often deal with chronic fatigue, cognitive difficulties, and hormonal imbalances, such as thyroid dysfunction or premature menopause. Permanent infertility is a frequent outcome due to the intensive conditioning treatments used before the transplant. Furthermore, there is an elevated risk of secondary cancers, including solid tumors, leukemia, or myelodysplastic syndromes, which may develop years after the procedure.
Complication Rate Comparison
Short-Term vs. Long-Term Complications
The recovery period after a transplant is a critical time, with outcomes heavily influenced by complications and how quickly the body recovers. Cord blood and bone marrow transplants show clear differences in their complication profiles during this phase. One of the most notable contrasts is in early infection risk. Cord blood recipients face a significantly higher risk of infections in the first 100 days, with infection-related deaths reaching 45% for mismatched cord blood transplants. In comparison, bone marrow recipients experience a much lower rate, at 21–24%. This disparity stems from cord blood's slower neutrophil recovery - taking a median of 27 days versus 18–20 days for bone marrow - leaving recipients more vulnerable to infections early on.
On the other hand, cord blood transplants shine when it comes to chronic Graft-Versus-Host Disease (GVHD). While both types of transplants carry a moderate risk for acute GVHD, cord blood has a clear advantage in reducing chronic GVHD. Extensive chronic GVHD affects only 33% of cord blood recipients, a stark contrast to the 52–71% seen in bone marrow recipients. This lower rate of chronic GVHD significantly enhances long-term quality of life for cord blood transplant patients.
Another key difference lies in immune recovery timelines. Bone marrow transplants typically achieve full immune reconstitution within 6–18 months, while cord blood takes slightly longer, ranging from 6–24 months. This extended recovery window for cord blood contributes to its higher early infection risk. However, beyond the initial 100 days, long-term infection risks tend to even out between the two transplant types.
Graft rejection is another factor to consider. The risk of rejection is moderate-to-high for cord blood transplants compared to low-to-moderate for bone marrow. Despite cord blood's immunological naivety - which helps lower GVHD risk - it ironically increases the likelihood of graft rejection. This can complicate recovery, potentially requiring additional treatments or even a second transplant. As the National Cancer Institute points out, "defective immune reconstitution is a major barrier to successful HSCT, regardless of graft source", highlighting the need for careful management in either case.
The Role of Newborn Stem Cell Banking
Benefits of Cord Blood Banking
Banking your baby's cord blood at birth offers a safeguard that could be life-saving in critical moments. While cord blood transplants might initially involve slower recovery and higher infection risks, having these cells stored ensures they're ready for immediate use if needed. This eliminates delays tied to searching for a donor, making timely treatment possible when every moment counts.
The benefits go even further when cord blood and cord tissue are stored together. Cord blood contains hematopoietic stem cells (HSCs), which are vital for regenerating blood and immune systems. Meanwhile, cord tissue and placental tissue are rich in mesenchymal stem cells (MSCs), which aid in tissue repair and reduce inflammation. Research published in the Transplantation Journal highlights that combining these cells during transplantation can shorten engraftment time and boost recovery, helping the body heal faster after the procedure.
Advanced processing methods also play a key role. Americord's CryoMaxx™ processing system is designed to maximize the number of viable stem cells by isolating them effectively. Their use of 5-compartment storage bags allows for targeted cell usage during treatments while keeping the remaining cells intact for future needs. This flexibility is a game-changer compared to single-use storage.
Americord Registry's Approach

Americord Registry takes these advantages a step further by offering cutting-edge preservation methods that retain the natural therapeutic properties of the cells. Their services include banking for cord blood, cord tissue, placental tissue, and exosomes, all processed with minimal manipulation to maintain essential components like growth factors and cytokines.
Americord supports their services with a $110,000 Cord Blood Quality Guarantee and adheres to AABB-accredited laboratory standards. Pricing starts at $3,799 for cord blood banking, with payment plans as low as $131 per month, making it an accessible option for families looking to secure these resources at birth.
As Dr. Jonathan Gutman from the University of Colorado Denver observed in his research on transplant outcomes: "When you look past the first 100 days - a point at which many centers stop collecting data - there is clear evidence that cord blood outperforms cells from matched, unrelated donors."
Conclusion
Cord blood and bone marrow transplants each come with their own set of advantages. Bone marrow transplants generally lead to faster recovery times - engraftment takes about 18 days for neutrophils and 29 days for platelets. On the other hand, cord blood transplants, while slower to engraft (27 days for neutrophils and 60 days for platelets), drastically lower the risk of severe GVHD. For example, unrelated bone marrow transplants carry a 60% risk, compared to just 10% in autologous cord blood cases. This is largely due to the immature immune cells in cord blood, which can improve long-term quality of life.
However, the slower engraftment of cord blood does come with an increased risk of early infections, though this risk levels out over time. Interestingly, research shows that survival and mortality rates are comparable between mismatched cord blood and mismatched bone marrow transplants. Cord blood also offers a logistical advantage - it’s banked and ready for immediate use, unlike bone marrow, which requires finding a compatible donor, a process that can delay treatment when time is critical.
There’s also the added benefit of genetic compatibility. Cord blood stored at birth guarantees a perfect match for the infant and increases the likelihood of compatibility for siblings and other relatives. With over 80 FDA-approved treatments and more than 300 ongoing clinical trials investigating new uses, the possibilities for cord blood therapy continue to grow.
These factors - recovery times, risks, and practical benefits - help families weigh their options when considering stem cell banking. Choosing to bank cord blood provides a valuable resource that could play a crucial role in addressing future health challenges.
Discover how you can take this step toward securing your family’s health with Americord Registry.
FAQs
How do recovery times differ between cord blood and bone marrow transplants?
Recovery times for cord blood and bone marrow transplants mainly differ in how quickly the body starts producing healthy blood cells, a process called engraftment. With cord blood transplants, engraftment generally takes around 3 to 5 weeks. In contrast, bone marrow transplants typically take about 2 to 3 weeks.
The longer engraftment period associated with cord blood can lead to a slower recovery of blood cell counts and an extended period of immune suppression. Despite this, cord blood offers distinct benefits, such as a reduced risk of complications like graft-versus-host disease, making it a viable choice for some patients.
How does the risk of Graft-Versus-Host Disease differ between cord blood and bone marrow transplants?
The likelihood of experiencing Graft-Versus-Host Disease (GVHD) is much lower with cord blood transplants compared to bone marrow transplants. Research highlights a stark difference: the incidence of GVHD in cord blood transplants can be as low as 8%, whereas it reaches nearly 48% in bone marrow transplants involving unrelated donors.
Although recovery of blood cell counts may take longer with cord blood transplants, the reduced severity of GVHD significantly lowers the chances of enduring long-term complications. This makes cord blood an important option for patients who want stem cell therapies with fewer immune-related risks.
Why might someone choose cord blood over bone marrow for a transplant, even if recovery takes longer?
Cord blood is often preferred over bone marrow for transplants due to its distinct advantages, even though recovery might take longer. One major benefit is that cord blood stem cells carry a lower risk of graft-versus-host disease (GVHD), a serious complication that can occur after a transplant. This reduced risk makes cord blood a safer choice for patients where GVHD is a significant concern.
Another key advantage is accessibility. Cord blood can be stored ahead of time, ensuring it's available when needed. On the other hand, locating a compatible bone marrow donor can take months, potentially delaying urgent treatment. These factors highlight why cord blood is an important option for certain patients, even with its slower recovery timeline.
The views, statements, and pricing expressed are deemed reliable as of the published date. Articles may not reflect current pricing, offerings, or recent innovations.


